The Impact Of Famines On South Asian Epigenetics
The prevalence of cardiometabolic diseases in South Asians, as compared to other ethnic groups, was first explored in the 1950s. Scientists in Singapore studied global and national mortality data to compare the mortality rates of different ethnic groups for coronary heart disease (Danaraj et al., 1959). Their research was an early indicator that South Asians may be more susceptible than other ethnic groups to certain cardiometabolic diseases. This laid the groundwork for more research pertaining to the link between ethnicity and cardiometabolic risk.

Decadal Deaths from Famines by Region (1870–2023)
This graph illustrates the estimated number of deaths from famines that claimed at least 100,000 lives per decade, highlighting the disproportionate burden borne by Asia—particularly South Asia—during the 19th and 20th centuries. The sharp spikes in the 1870s, 1940s, and 1960s correspond to periods of extreme food scarcity, including multiple famines during British colonial rule in India. These repeated famine exposures are now being studied for their potential long-term effects on the region’s epigenetics, metabolism, and disease susceptibility.Source: World Peace Foundation (2025), via OurWorldInData.org
An increasing number of ethnicity-based studies gained prominence during the 1980s and 1990s, a trend strongly correlated to the mass migration of South Asians to first world countries. Comparative studies were conducted in Europe and North America, aiming to understand the unique health profiles of South Asians. The objective was to enable healthcare systems to improve diagnosis and treatment outcomes for various subgroups (Volgman et al., 2018), ultimately leading to a healthier overall population.
Current data suggests that South Asians are 4-5 times more likely to suffer from type 2 diabetes as compared to White populations in the US and the UK (Syed, 2022). Additionally, population research from Imperial College London suggests that South Asians at every age group have a 1.7-fold higher risk of developing coronary heart disease as compared to their White counterparts of European descent (Mehta, 2024).
This Begs The Question: Why Is There Such a Substantial Gap?
There are several research papers suggesting that lifestyle choices such as the lack of sufficient exercise and traditional carbohydrate-rich diets are major risk factors for South Asians. However, epigenetics studies suggest that there is more to this than conventional risk factors like diet and exercise (Syed, 2022).
So, Why Is This Subgroup Particularly More Susceptible To Cardiometabolic Diseases?
To understand this, we must go back in time and examine the history of famines in South Asia, and how these events shaped South Asian epigenetics.
During the British rule in India (1765-1947), the frequency and severity of famines increased in the Indian subcontinent. During this period, some historians recorded 25 major famines, with an estimated death toll of 60 million people (Purkait et al., 2020), while others documented 31 major famines (Syed, 2022). An increase in undernourishment was marked during the Second World War, as food grain availability per capita decreased from 200 kg to 137 kg (Syed, 2022).
Exposure to even a single famine can elevate the risk of cardiometabolic diseases in a population, potentially by triggering transgenerational epigenetic changes (Syed, 2022).
But What Are The Consequences When A Population Suffers Through Not Just 1, But 25 Such Famines?
To understand this, I’m going to delve into two relevant hypotheses - the thrifty gene hypothesis and the starvation adaptation hypothesis.
The Thrifty Gene Hypothesis:
This hypothesis employs the principle of good old-fashioned natural selection to explain why certain populations (such as South Asians) that have undergone famines may select for traits that helped them better survive long periods of undernourishment and starvation. It states that there are ‘thrifty alleles’ of genes that store fat more easily and thus increase the rate of survival through famines (Syed, 2022). This makes sense from an evolutionary point of view; we improvise, and we survive, right?
This hypothesis was further explored by studying various genetic variations to identify these so-called ‘thrifty genes’. Let’s examine two genes most widely studied in this theory— MC4R and FTO genes.
MC4R Gene:
Animal studies in the late 1990s revealed that the MC4R gene may be linked to obesity, suggesting that it may have an important role in regulating body weight. With the advent of new technologies and methods such as Genome-Wide Association Studies (GWAS), scientists discovered that South Asians have a higher prevalence of genetic variants near the gene MC4R. Simply put, South Asians are more prone to having higher abdominal fat storage and increased waist circumference, which are risk factors for obesity and insulin resistance (Chambers et al., 2008).
FTO Gene:
Similarly, the FTO gene has also been found to be directly linked to the regulation of body weight, energy balance, and appetite control. Several studies have confirmed that multiple variants of FTO gene have a key role in increasing the risk of type 2 diabetes and obesity in South Asians (Ramya et al., 2011).
These genetic variations, specifically detected in South Asians, suggest that these genes may have acted ‘thrifty’ in environments that required that change. According to this hypothesis, these genetic variations that increase fat storage and insulin resistance were preferred during times of food scarcity (Syed, 2022).
If we look at the 21st century of improved global food security and sedentary lifestyles, we do not require superior fat storing abilities, in fact, we prefer the opposite. As we see a rise in the number of cases of type 2 diabetes, obesity and heart disease in South Asians, we can safely conclude that the traits they once needed to survive are the ones now harming them.
This hypothesis has been tested out in various animal and human studies through the years. While some of these studies have shown a promising result for the hypothesis (Myles et al., 2011), the consensus is inconclusive as more genetic research is required to prove it indefinitely (Syed, 2022). The thrifty gene hypothesis has not been conclusively validated yet in the field of genetic. Additionally, cardiometabolic diseases and their causations are far more complex to have a singular evolutionary explanation.
Starvation Adaptation Hypothesis:
Another famous hypothesis in the spotlight is the “starvation adaptation hypothesis” which essentially conveys the same meaning as the thrifty gene hypothesis. This hypothesis states that due to repeated exposure to famines, the population underwent various physiological changes to adapt to that environment. The only difference between the two hypotheses is that starvation adaptation hypothesis talks about physiological changes in humans while the former talks about genetic changes (Syed, 2022).
Resting Energy Expenditure:
One of the physiological changes associated with this hypothesis is the level of resting energy expenditure. South Asians tend to have lower resting energy expenditure than Caucasians (Wulan et al., 2021). Resting energy expenditure or resting metabolic rate refers to the expenditure of energy for vital activities that happen while our bodies are at rest, such as keeping your organs always working (Westerterp, 2000). This points to the fact that South Asians burn less energy at rest as compared to Caucasians, which according to the hypothesis may have been an adaptive trait to survive famines (Syed, 2022).
Obesity:
We already know that obesity increases the risk for cardiometabolic diseases like cardiovascular diseases and type 2 diabetes. What’s more is that South Asians have an increased risk of developing these metabolic diseases at a considerably lower BMI threshold than their White counterparts. Because of this, the World Health Organisation has recommended lower BMI cutoff numbers to be specified for South Asians for a more accurate diagnosis of obesity (Gupta, Brister, & Verma, 2006).
This is mainly because fat storage and body composition differ in this subgroup.
South Asians are known to have a “thin fat phenotype”, which basically refers to an individual with a normal body weight having abnormally high amounts of fat stored in the abdominal area and thus low overall muscle mass. In fact, one study concluded that South Asians had significantly higher levels of total abdominal fat than their White counterparts having similar BMI levels (Raji et al., 2001). This unique body composition means that South Asians may have underlying metabolic issues that could be missed due to their low BMI which may not meet the cut off for obesity diagnosis (Syed, 2022). According to the hypothesis, this unique fat storage and body composition has been posed as a potential physiological change caused by exposure to famines, as this type of fat storage would be beneficial during long periods of starvation (Syed, 2022).

Ethnic Differences in Body Fat Distribution and Metabolic Markers
This figure compares various metabolic and fat distribution parameters between South Asian and Caucasian men. While total body fat and fat mass did not differ significantly, South Asians exhibited significantly larger subcutaneous adipocytes, lower glucose disposal rates (a marker of insulin sensitivity), and reduced plasma adiponectin levels—all associated with higher metabolic risk. These findings suggest that despite similar levels of adiposity, South Asians may have a distinct fat biology that contributes to greater insulin resistance, potentially influenced by both genetic and historical environmental factors such as famine exposure. Source: Chandalia et al., 2003, via Semantic Scholar
Low Muscle Mass & High Fat Storage:
South Asians have lower muscle mass as compared to other population groups, especially when compared to groups of European descent (Syed, 2022). Research suggests that South Asians exhibit a higher expression of the myostatin gene, encoding to produce Myostatin, a protein that inhibits muscle growth (Narayan & Kanaya, 2020). It is commonly hypothesized that because of natural selection, South Asians experiencing famines have selected for higher expression of myostatin protein. This is simply because muscle tissue consumes more energy in the body than fat tissue. So, to be ‘thrifty’ and preserve energy most efficiently, it is hypothesized that the myostatin gene was selected for survival (Syed, 2022). While most of the current research points towards South Asians having genetic variations of the myostatin gene that account for their unique body composition, we need more South Asian focused studies to conclusively prove that this subgroup consistently has higher expression of myostatin.
Insulin Resistance:
Our muscles need glucose to maintain themselves and insulin is the key hormone that helps cells absorb it. Our muscles account for most of our overall insulin uptake, so what happens when we have low overall muscle mass? There’s an increase in blood glucose levels because glucose has nowhere to go and get absorbed. There is a decrease in insulin sensitivity, creating insulin resistance in muscle tissue which is the perfect environment for the occurrence of type 2 diabetes (Liu & Zhu, 2023). Hence, having low muscle mass is a common risk factor for higher insulin resistance, which in turn increases the risk for type 2 diabetes (Syed, 2022).
The starvation adaptation hypothesis suggests that factors such as lower resting energy expenditure, increased abdominal fat storage and lower lean muscle mass are physiological changes that manifested because of starvation adaptation, leading to an increased risk of obesity and insulin resistance (Syed, 2022).
For now, these hypotheses have not been proven to be true. Considerable research is needed to prove that the positive selection of certain genes or the manifestation of certain physiological changes have been triggered by environmental factors like famines, leading to an increased risk in cardiometabolic diseases.
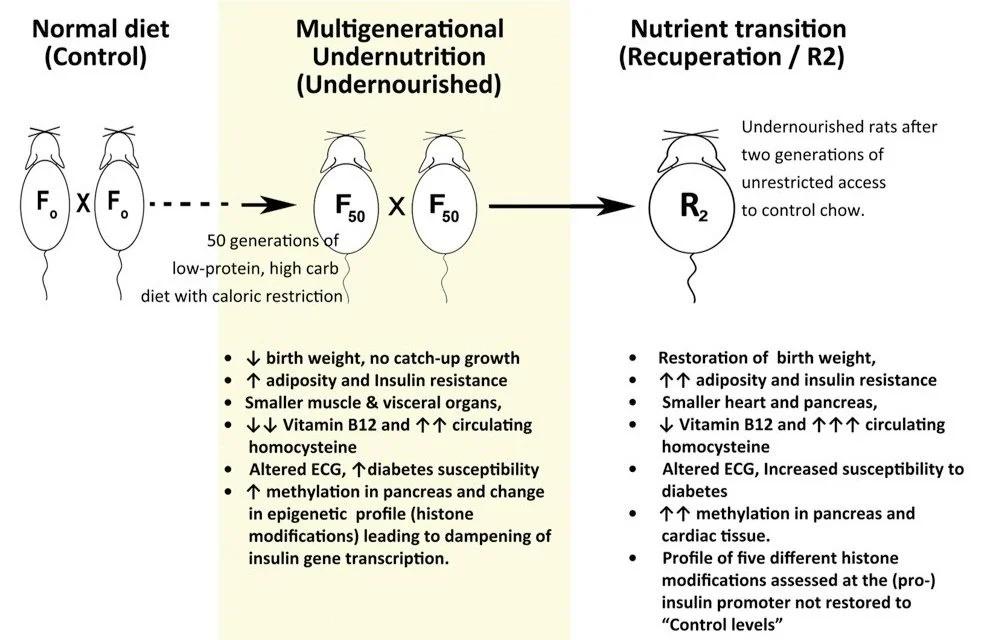
Animal Studies Replicating Famine Conditions:
Ethnic Differences in Body Fat Distribution and Metabolic Markers
This figure compares various metabolic and fat distribution parameters between South Asian and Caucasian men. While total body fat and fat mass did not differ significantly, South Asians exhibited significantly larger subcutaneous adipocytes, lower glucose disposal rates (a marker of insulin sensitivity), and reduced plasma adiponectin levels—all associated with higher metabolic risk. These findings suggest that despite similar levels of adiposity, South Asians may have a distinct fat biology that contributes to greater insulin resistance, potentially influenced by both genetic and historical environmental factors such as famine exposure. Source: Chandalia et al., 2003, via Semantic Scholar
I’d like to talk about a particularly interesting animal study by Hardikar et al. (2015) involving rats that underwent undernourishment for 50 generations. The rats developed a very similar phenotype to undernourished humans with famine histories. The observed phenotype included low birth weights, insulin resistance, increased abdominal fat, nutritional deficiencies and increased susceptibility to diabetes. Additionally, these rats were then re-introduced to their standard diets for two generations to study if any kind of reversal effects would take place. The results concluded that the abnormal metabolic changes could not be reversed in the second-generation following nutritional rehabilitation.
Future Considerations:
An interesting statistic to note is that South Asians make up a quarter of the global population, but 60% of global cardiovascular disease cases occur in India alone.
While behavioural risk factors such as smoking, diet, physical activity may increase the risk of cardiometabolic diseases in humans (Shah et al., 2022), it is important to note that South Asians have unique genetics that will exacerbate the effects of these risk factors (Palaniappan et al., 2018). Hence, we need better healthcare measures for such a prominently large population, focusing on both prevention and treatment.
More large-scale genome studies and population studies are needed to determine epigenetic markers and risk assessment factors such as polygenic risk scores (Sun et al., 2021). Such ethnicity-based studies will lead to timely diagnosis through improved risk stratification, which may improve survival rates in surgeries.
In terms of better treatment for South Asians, further research can help pave the path for personalised medication and improved drug therapy that are targeted for their unique genetic and metabolic profile (Palaniappan et al., 2018).
-
· Chambers, J. C., Elliott, P., Zabaneh, D., Zhang, W., Li, Y., Froguel, P., Balding, D., Scott, J., & Kooner, J. S. (2008). Common genetic variation near MC4R is associated with waist circumference and insulin resistance. Nature Genetics, 40(6), 716–718. https://doi.org/10.1038/ng.156
· Danaraj, T. J., Acker, M. S., Danaraj, W., Ong, W. H., & Yam, T. B. (1959). Ethnic group differences in coronary heart disease in Singapore: An analysis of necropsy records. American Heart Journal, 58(4), 516–526. https://doi.org/10.1016/0002-8703(59)90085-7
· DIAGRAM, MuTHER, Kooner, J. S., Saleheen, D., Sim, X., Sehmi, J., Zhang, W., Frossard, P., Been, L. F., Chia, K.-S., Dimas, A. S., Hassanali, N., Jafar, T., Jowett, J. B. M., Li, X., Radha, V., Rees, S. D., Takeuchi, F., Young, R., … Chambers, J. C. (2011a). Genome-wide association study in individuals of South Asian ancestry identifies six new type 2 diabetes susceptibility loci. Nature Genetics, 43(10), 984–989. https://doi.org/10.1038/ng.921
· Gupta, M., Brister, S., & Verma, S. (2006). Is South Asian ethnicity an independent cardiovascular risk factor? Canadian Journal of Cardiology, 22(3), 193–197. https://doi.org/10.1016/S0828-282X(06)70895-9
· Hardikar, A. A., Satoor, S. N., Karandikar, M. S., Joglekar, M. V., Puranik, A. S., Wong, W., Kumar, S., Limaye, A., Bhat, D. S., Januszewski, A. S., Umrani, M. R., Ranjan, A. K., Apte, K., Yajnik, P., Bhonde, R. R., Galande, S., Keech, A. C., Jenkins, A. J., & Yajnik, C. S. (2015). Multigenerational undernutrition increases susceptibility to obesity and diabetes that is not reversed after dietary recuperation. Cell Metabolism, 22(2), 312–319. https://doi.org/10.1016/j.cmet.2015.06.008
· Liu, Z., & Zhu, C. (2023). Causal relationship between insulin resistance and sarcopenia. Diabetology & Metabolic Syndrome, 15(1), 46. https://doi.org/10.1186/s13098-023-01022-z
· Mehta, K. (2024, June 5). South Asians almost twice as likely to develop coronary heart disease than White Europeans. British Heart Foundation. https://www.bhf.org.uk/what-we-do/news-from-the-bhf/news-archive/2024/june/south-asians-almost-twice-as-likely-to-develop-coronary-heart-disease-than-white-europeans
· Myles, S., Lea, R. A., Ohashi, J., Chambers, G. K., Weiss, J. G., Hardouin, E., Engelken, J., Macartney-Coxson, D. P., Eccles, D. A., Naka, I., Kimura, R., Inaoka, T., Matsumura, Y., & Stoneking, M. (2011). Testing the thrifty gene hypothesis: The Gly482Ser variant in PPARGC1Ais associated with BMI in Tongans. BMC Medical Genetics, 12(1), 10. https://doi.org/10.1186/1471-2350-12-10
· Narayan, K. M. V., & Kanaya, A. M. (2020). Why are South Asians prone to type 2 diabetes? A hypothesis based on underexplored pathways. Diabetologia, 63(6), 1103–1109. https://doi.org/10.1007/s00125-020-05132-5
· Palaniappan, L., Garg, A., Enas, E., Lewis, H., Bari, S., Gulati, M., Flores, C., Mathur, A., Molina, C., Narula, J., Rahman, S., Leng, J., & Gany, F. (2018). South asian cardiovascular disease & cancer risk: Genetics & pathophysiology. Journal of Community Health, 43(6), 1100–1114. https://doi.org/10.1007/s10900-018-0527-8
· Purkait, P., Kumar, N., Sahani, R., & Mukherjee Sumit, S. (2020). Major famines in india during british rule: A referral map.
· Raji, A., Seely, E. W., Arky, R. A., & Simonson, D. C. (2001). Body fat distribution and insulin resistance in healthy asian indians and caucasians. The Journal of Clinical Endocrinology & Metabolism, 86(11), 5366–5371. https://doi.org/10.1210/jcem.86.11.7992
· Ramya, K., Radha, V., Ghosh, S., Majumder, P. P., & Mohan, V. (2011). Genetic variations in the fto gene are associated with type 2 diabetes and obesity in south indians(CURES-79). Diabetes Technology & Therapeutics, 13(1), 33–42. https://doi.org/10.1089/dia.2010.0071
· Shah, K. S., Patel, J., Al Rifai, M., Agarwala, A., Bhatt, A. B., Levitzky, Y. S., & Palaniappan, L. (2022). Cardiovascular risk management in the south asian patient: A review. Health Sciences Review, 4, 100045. https://doi.org/10.1016/j.hsr.2022.100045
· Sun, Y. V., Liu, C., Staimez, L., Ali, M. K., Chang, H., Kondal, D., Patel, S., Jones, D., Mohan, V., Tandon, N., Prabhakaran, D., Quyyumi, A. A., Narayan, K. M. V., & Agrawal, A. (2021). Cardiovascular disease risk and pathophysiology in South Asians: Can longitudinal multi-omics shed light? Wellcome Open Research, 5, 255. https://doi.org/10.12688/wellcomeopenres.16336.2
· Syed, M. (2022). The susceptibility of south asians to cardiometabolic disease as a result of starvation adaptation exacerbated during the colonial famines. Endocrinology, Diabetes and Metabolism Journal, 6(2). https://doi.org/10.31038/EDMJ.2022621
· The susceptibility of south asians to cardiometabolic disease as a result of starvation adaptation exacerbated during the colonial famines. (2022). Endocrinology, Diabetes and Metabolism Journal, 6(2). https://doi.org/10.31038/EDMJ.2022621
· Volgman, A. S., Palaniappan, L. S., Aggarwal, N. T., Gupta, M., Khandelwal, A., Krishnan, A. V., Lichtman, J. H., Mehta, L. S., Patel, H. N., Shah, K. S., Shah, S. H., Watson, K. E., & On behalf of the American Heart Association Council on Epidemiology and Prevention; Cardiovascular Disease and Stroke in Women and Special Populations Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Quality of Care and Outcomes Research; and Stroke Council. (2018). Atherosclerotic cardiovascular disease in south asians in the united states: Epidemiology, risk factors, and treatments: a scientific statement from the american heart association. Circulation, 138(1). https://doi.org/10.1161/CIR.0000000000000580
· Westerterp, K. R. (2000). Control of energy expenditure in humans. In K. R. Feingold, S. F. Ahmed, B. Anawalt, M. R. Blackman, A. Boyce, G. Chrousos, E. Corpas, W. W. de Herder, K. Dhatariya, K. Dungan, J. Hofland, S. Kalra, G. Kaltsas, N. Kapoor, C. Koch, P. Kopp, M. Korbonits, C. S. Kovacs, W. Kuohung, … D. P. Wilson (Eds.), Endotext. MDText.com, Inc. http://www.ncbi.nlm.nih.gov/books/NBK278963/
· Wulan, S. N., Raza, Q., Prasmita, H. S., Martati, E., Maligan, J. M., Mageshwari, U., Fatima, I., & Plasqui, G. (2021). Energy metabolism in relation to diet and physical activity: A south asian perspective. Nutrients, 13(11), 3776. https://doi.org/10.3390/nu13113776